Early Intervention, Causes, Casting, and Surgical Management
1. Introduction
Clubfoot is a congenital deformity present at birth in which the foot is twisted inward and downward. It may affect one or both feet and, if untreated, can lead to long-term disability and abnormal walking patterns. With early and appropriate treatment, most children achieve near-normal function and mobility.

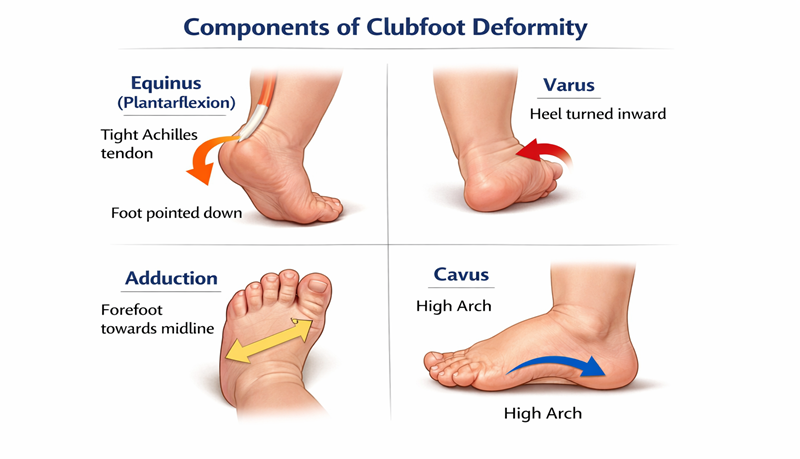
2. Components of the Deformity
Equinus – plantarflexion at the ankle joint
Varus – inward turning of the heel
Adduction – forefoot deviates toward the midline
Cavus – high medial longitudinal arch
3. Causes of Clubfoot
Idiopathic causes (most common)
Genetic factors
Neuromuscular causes (e.g., cerebral palsy, spina bifida)
Syndromic causes (e.g., arthrogryposis)
Intrauterine factors
4. Importance of Early Intervention
Treatment should begin within 1–2 weeks after birth. Early management allows easier correction and prevents long-term disability.
5. Ponseti Method
Phase 1: Manipulation and casting (5–8 weeks)
Phase 2: Achilles tenotomy
Phase 3: Bracing (up to 3–4 years)
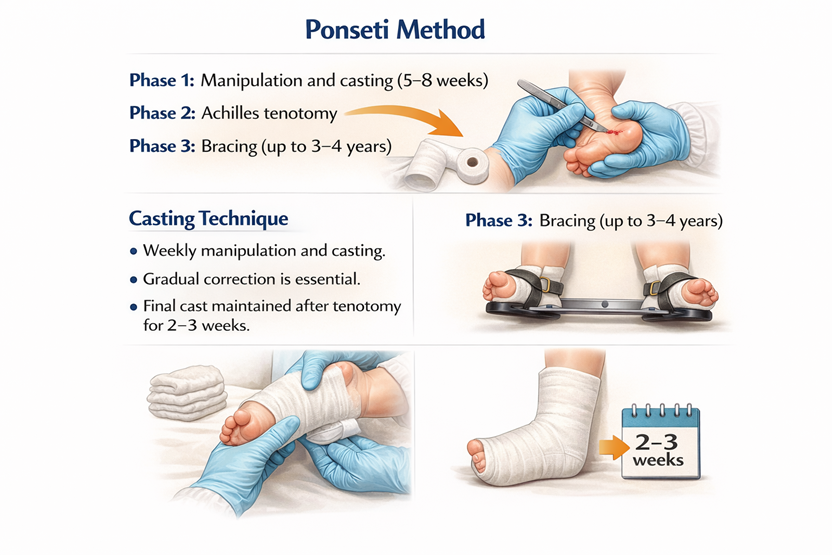
6. Casting Technique
Weekly manipulation and casting. Gradual correction is essential. Final cast maintained after tenotomy for 2–3 weeks.

7. Indications for Surgery
Failure of casting
Late presentation
Recurrent deformity
Severe or syndromic cases
8. Types of Surgery
Achilles tenotomy
Tendon transfer
Soft tissue release
Bony procedures
9. Complications and Recurrence
Recurrence due to poor brace compliance
Mild stiffness or calf atrophy
10. Role of Physiotherapy
Stretching exercises
Parental education
Gait training
11. Conclusion
Early diagnosis and treatment of clubfoot lead to excellent outcomes. The Ponseti method remains the gold standard.