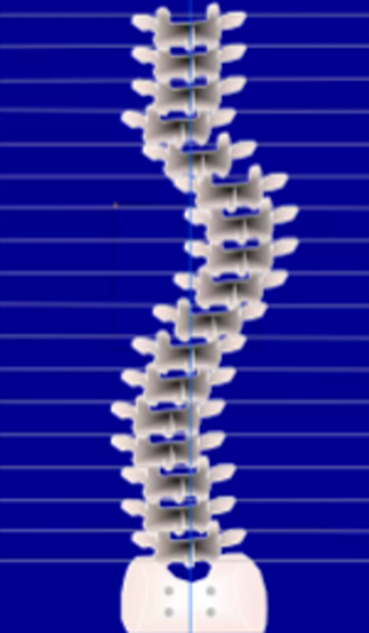
- “Scoliosis” -Greek word meaning “crooked”.
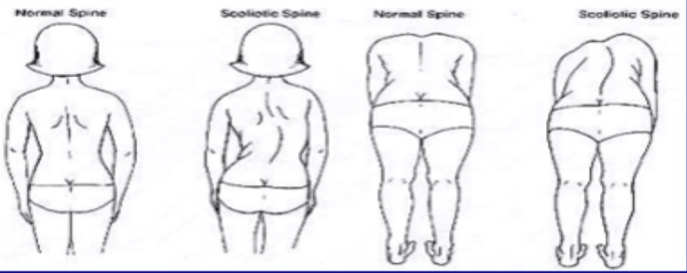
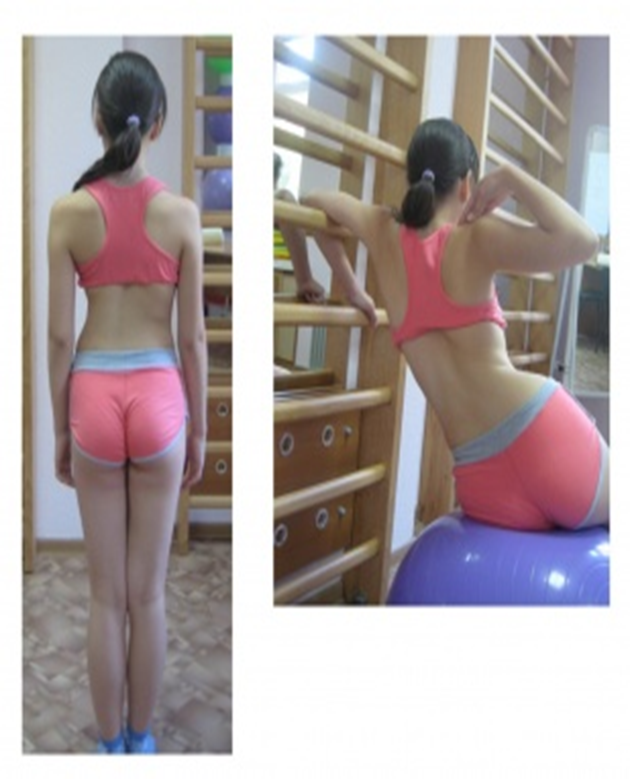
- It is a lateral curvature of the spine in upright position.
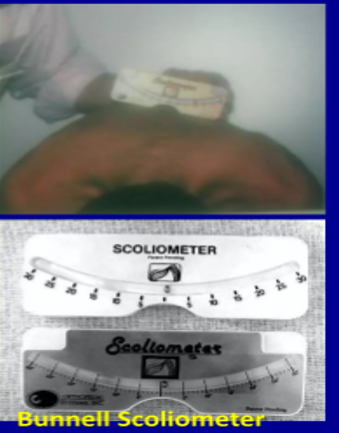
- The Scoliosis Research Society has defined scoliosis as a lateral curvature of the spine greater than 10 degree as measured using the Cobbs method on a standing radiograph.
- Triplanar deformity of lordosis, rotation & lateral wedging of vertebrae.
- It produces body disfigurement. When deformity is extreme it compresses viscera & reduces life expectancy of the patient.

Incidence of scoliosis:
- Develops between ages 8-15.
- 7 times more prevalent in females.
- 80%of scoliosis orign unknown.
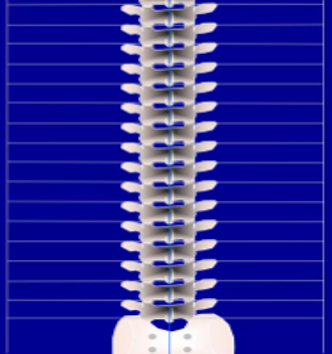
Spinal Biomechanics:
- “Normal” alignment
Spinous processes all lined up in a straight line up in a straight over the sacrum.
- Scoliosis is a combination of
Angular displacement
Lateral displacement.





About Authors
Dr. Muhammad Mahmood Ahmad is a Spinal as well as an Orthopedic Surgeon with over 14 years of experience currently practicing at Razia Saeed Hospital, Multan.